
"Colcrys 0.5mg generic, virus protection".
By: S. Nerusul, MD
Co-Director, Western University of Health Sciences
He is on the Editorial Boards of Clinical Nephrology treatment for uti yahoo 0.5mg colcrys with amex, Peritoneal Dialysis International antibiotic eye drops for conjunctivitis buy colcrys with a visa, Nephron Clinical Practice virus del nilo buy colcrys 0.5 mg, Chinese Journal of Nephrology antibiotics safe while breastfeeding cheapest colcrys, Dialysis & Transplantation, Medical Progress, Indian Journal of Peritoneal Dialysis, and is a regular reviewer for all the major nephrology journals. He has published over 380 original and review articles in peerreviewed journals, two books and 17 book chapters, and has given lectures to over 100 international congresses and meetings. Liu was appointed Professor of Medicine at Nanjing University in 1996 and became Adjunct Professor of Medicine at Brown University in 2008. She has published 390 articles, authored two books, and contributed chapters to nephrology textbooks. Liu also served on the editorial boards of several peer-reviewed journals, including as editorin-chief of the Chinese Journal of Nephrology Dialysis & Transplantation. She was honored with the National Science and Technology Progress Award of China; the National Young Investigator Award and National Outstanding Individual Award in Science and Technology from the China Association for Science and Technology; and the Guanghua Engineering & Technological Science Award from Chinese Academy of Engineering. Liu directs one of the most productive renal patient care and research programs in China, the Research Institute of Nephrology, Jinling Hospital at the Nanjing University School of Medicine and she is the Board member of Academic Degrees Committee, Nanjing University. Liu has served on several international committees related to scientific programs and global scientific interactions and she worked as Scientific Program Committee member of the World Congress of Nephrology in 2007. He has served as Past President of both the Chilean Society of Nephrology (1996-1998) and Latin American Society of Nephrology (2002-2004). He graduated from Boston University School of Medicine and received fellowship training at University of North Carolina at Chapel Hill. As an author of over 50 publications, he maintains a firm commitment to postgraduate education both at the national and international level. Nachman was awarded the Internal Medicine Housestaff Faculty Award in 2007 and acknowledged in Best Doctors in America from 20082010. He is member of the Scientific Committee at the ``Instituto ґ de Investigacion Hospital 12 de Octubre'. He obtained his medical degree from the University of Valladolid and completed a nephrology fellowship at Hospital Puerta de Hierro, Madrid, Spain. He has authored more than 200 peer-reviewed publications and numerous book chapters, and has received many awards, ~ including the ``Inigo Alvarez de Toledo' award to Clinical Investigation in 2000 and 2008. Praga has served on the Directory Board of the Spanish Society of Nephrology, and also sits as an editorial board member and reviewer for international journals. His current research activities focus on primary and secondary glomerular diseases, renal complications of obesity, diabetic nephropathy, role of proteinuria in the progression of renal damage, interstitial renal diseases, and renal transplantation. His clinical and research interests are therapy of glomerular diseases and intensive-care nephrology. He received his medical degree from University of Illinois and completed nephrology fellowship training at Washington University School of Medicine in St. Rovin has served on the editorial boards of American Journal of Kidney Disease, Clinical Nephrology, Journal of the American Society of Nephrology, Kidney International and as a manuscript reviewer for 16 other journals. Troyanov completed his medical studies at Universite ґ de Montreal and received fellowship training at University of Toronto, Canada. His earlier research centered on ascertaining the determinants of remission in proteinuria in primary glomerular disease. Troyanov received the Clinician Research Award ґ ґ twice from Fonds de la Recherche en Sante du Quebec, an ґ agency of the Government of Quebec, and the Young ґ ґ ґ ґ ґ Nephrologist Prize from Societe Quebecoise de Nephrologie. He undertook his training in Internal Medicine and Nephrology at the Radboud University Nijmegen Medical Center and later received his PhD in 1989. Since 1992, he has been working as a nephrologist and was appointed Professor of Nephrology in the Department of Nephrology at Radboud University Nijmegen in 2002. Professor Wetzels is committed to teaching and research, with an emphasis on the diagnosis and treatment of patients with glomerular diseases. In 1993, following postgraduate training in internal medicine, pathology and physiology, he was appointed Assistant Professor of Physiology at the University of Regensburg, Germany. Professor Eckardt is Subject Editor of Nephrology Dialysis Transplantation, and serves on the editorial board of several other journals. He has also authored book chapters and most recently served as a Co-Editor of the text Studies on Renal Disorders.
However antibiotics for pcos acne 0.5mg colcrys mastercard, they do strongly suggest that it may not be necessary to target blood glucose values antimicrobial nanotechnology buy 0.5 mg colcrys free shipping,140 mg/dL (7 infection 4 weeks after hysterectomy purchase discount colcrys online. This is the standard definition in outpatients and correlates with the initial threshold for the release of counterregulatory hormones most effective antibiotics for sinus infection purchase cheap colcrys. Severe hypoglycemia in hospitalized patients has been defined by many as,40 mg/dL (2. Both hyperglycemia and hypoglycemia among inpatients are associated with adverse short- and longterm outcomes. Once intravenous insulin is started, the glucose level should be maintained between 140180 mg/dL (7. Although strong evidence is lacking, lower glucose targets may be appropriate in select patients. Insulin infusion protocols with demonstrated safety and efficacy, resulting in low rates of hypoglycemia, are highly recommended (11). Noncritically Ill Patients Hyperglycemia in the hospital has been defined as any blood glucose. For the majority of noncritically ill patients treated with insulin, premeal glucose targets should generally be,140 mg/dL (7. To avoid hypoglycemia, consideration should be given to reassessing the insulin regimen if blood glucose levels fall below 100 mg/dL (5. There is some evidence that systematic attention to hyperglycemia in the emergency room leads to better glycemic control in the hospital for those subsequently admitted (14). Patients with a prior history of successful tight glycemic control in the outpatient setting who are clinically stable may be maintained with a glucose range below the aforementioned cut points. Conversely, higher glucose ranges may be acceptable in terminally ill patients or in patients with severe comorbidities, as well as in those in patient-care settings where frequent glucose monitoring or close nursing supervision is not feasible. When the patient is transitioned off intravenous insulin to subcutaneous therapy, precautions should be taken to prevent hyperglycemia (15,16). Outside of critical care units, scheduled subcutaneous insulin that delivers basal, nutritional, and correction components (basalbolus regimen) is recommended for patients with good nutritional intake. For patients with type 1 diabetes, dosing insulin solely based on premeal glucose levels does not account for basal insulin requirements or caloric intake, increasing both hypoglycemia and hyperglycemia risks and potentially leading to diabetic ketoacidosis. Typical dosing schemes are based on body weight, with some evidence that patients with renal insufficiency should be treated with lower doses (18). The reader is referred to publications and reviews that describe available insulin preparations and protocols and provide guidance in the use of insulin therapy in specific clinical settings, including parenteral nutrition (19), enteral tube feedings, and high-dose glucocorticoid therapy (11). A small study in general medicine and surgical wards showed that treatment with sitagliptin resulted in similar glycemic control as a basalbolus regimen in patients with type 2 diabetes who had an A1C,7. Further studies are needed to define the role of incretin mimetics in the inpatient management of hyperglycemia. Tracking such episodes and analyzing their causes are important quality-improvement activities (22). Involvement of appropriately trained specialists or specialty teams may reduce length of stay, improve glycemic control, and improve outcomes (11). As hospitals move to comply with "meaningful use" regulations for electronic health records, as mandated by the Health Information Technology for Economic and Clinical Health Act, efforts should be made to ensure that all components of structured insulin order sets are incorporated into electronic insulin order sets (23,24). To achieve glycemic targets associated with improved hospital outcomes, hospitals will need a multidisciplinary approach to develop insulin management protocols that effectively and safely enable achievement of glycemic targets (25). Diabetes self-management in the hospital may be appropriate for competent youth and adult patients who have a stable level of consciousness and reasonably stable daily insulin requirements, successfully conduct self-management of diabetes at home, have physical skills needed to successfully self-administer insulin and perform self-monitoring of blood glucose, have adequate oral intake, are proficient in carbohydrate counting, use multiple daily insulin injections or insulin pump therapy, and understand sick-day management. The patient and physician, in consultation with nursing staff, must agree that patient self-management is appropriate while hospitalized. It is important that nursing personnel document basal rates and bolus doses taken on a daily basis. Consistent carbohydrate meal plans are preferred by many hospitals as they facilitate matching the prandial insulin dose to the amount of carbohydrate consumed (27). Because of the complexity of nutrition issues in the hospital, a registered dietitian, knowledgeable and skilled in medical nutrition therapy, should serve as an inpatient team member.
Mycoplasma and Mycobacterium Leprae Ureaplasma Introduction Mycoplasma belongs to class Mollicutes (Mollis can antibiotics for uti delay your period colcrys 0.5mg without prescription, soft; cutis infection vaginal discharge purchase colcrys visa, skin) antibiotic 5 day pack order genuine colcrys, order Mycoplasmatales bacteria hpf in urinalysis discount colcrys 0.5 mg overnight delivery. This order contains four families- Mycoplasmataceae, Acholeplasmataceae, Spiroplasmataceae, and Anaplasmataceae; of which, most mycoplasma causing human infections belong to the family Mycoplasmataceae. Family Acholeplasmataceae includes mostly saprophytic mycoplasmas; these mycoplasmas do not require sterols as growth factor. Family Spiroplasmataceae includes mostly mycoplasmas, which are parasites of arthropods and plants; they require sterols as their growth factor. Family Anaplasmataceae contains mycoplasmas that are strict anaerobes and are found in the intestinal tract of cattle and sheep. At least 13 species of genera Mycoplasma and Ureaplasma are known to colonize or cause diseases in humans. The genus Mycoplasma contains the pathogens that use glucose or arginine, but do not utilize urea. These species occur as commensals, parasites, and pathogens of a variety of plant insects and mammalian hosts. Mycoplasma pneumoniae is the most important species known to cause infection in humans. Mycoplasma hominis, Mycoplasma fermentans, Mycoplasma pirum, Mycoplasma salivarium, Mycoplasma orale, and Mycoplasma genitalium are the other pathogens that are commonly associated with human infections. Genus Ureaplasma consists of 5 species of which Ureaplasma urealyticum is the most important species isolated from infections of genital and respiratory tract in humans (Table 45-1). Properties of the Bacteria Morphology Mycoplasmas are very small bacteria measuring 150250 nm in dimension. Mycoplasma species was also considered to be L form of bacteria because they lack a cell wall. However, they differ from bacteria including L forms in the following properties: They have sterols in the cell membrane. Mycoplasmas show the following morphological features: Mycoplasmas are prokaryotes, but they differ from prokaryotes by having a unique cell membrane that contains sterols. Mycoplasma pathogens when first discovered were thought to be viruses or L form of bacteria. The absence of cell wall makes Mycoplasma resistant to penicillins, cephalosporins, vancomycin, and other antibiotics that interfere with the synthesis of the cell wall. Mycoplasma species typically show pleomorphism and occur as granular and filaments of various sizes. However, genomic replication and cell division are often asynchronous, resulting in production of multinucleate fragments and other body forms and chains of beads. These colonies do not show any thin hallow unlike that of fried-egg appearance colonies. Mycoplasmas do not have the capability to synthesize cholesterol and related sterols; hence these are supplied from outside for growth of mycoplasmas. The high concentration of animal serum (horse serum) is used as a source of exogenous sterols (cholesterol and other lipids). The medium is supplemented with penicillin, ampicillin, and polymyxin B to inhibit growth of contaminating bacteria, and amphotericin B is used to inhibit contamination with fungi. Initially, the mycoplasmas multiply within the agar to produce opaque, ball-shaped colonies that grow up to the surface of the agar and then spread around it, forming a translucent peripheral zone. By this staining, the fried-egg appearance colonies of mycoplasma appear highly granular, with the center of the colonies stained dark blue and the periphery of the colonies staining light blue. The liquid culture medium used for fermentation reaction is supplemented with glucose, arginine, and urea, and phenol red as an indicator. Mycoplasma species fermenting carbohydrate utilize glucose to produce lactic acid, resulting in formation of acidic pH. Chapter 45 Other properties Susceptibility to physical and chemical agents: Mycoplasmas are readily killed by heating at 56°C for 30 minutes. The bacteria are sensitive to antiseptic solutions, such as cycloheximide and cetrimide, which inhibit their growth.

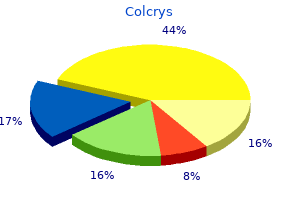
The infected individual is contagious from one to two days before appearance of the vesicles antibiotics for uti how long to take buy generic colcrys from india. Varicella is more serious in adults and immunocompromised patients virus 07 cheap colcrys 0.5mg line, potentially causing pneumonia antibiotic 875 order colcrys with paypal, fulminant hepatic failure antibiotics for acne buy online buy generic colcrys 0.5 mg line, and varicella encephalitis. Fetal infection during pregnancy is uncommon, but can result in multiple developmental anomalies. Treatment of primary varicella in immunocompromised patients, adults, and neonates is warranted by the severity of the disease. Famciclovir, given early in the acute phase of zoster, decreases acute pain and the time to resolution of lesions, and also shortens the duration of postherpetic pain. Varicellazoster immune globulin can protect neonates and immunocompromised individuals who have been exposed to chickenpox or zoster lesion fluid. On reactivation, there is substantial multiplication and horizontal spread of virus among the cells in the ganglion. Viral destruction of sensory ganglia leads to the pain associated with acute zoster. Debilitating postherpetic neuralgia and abnormal sensory phenomena may last as long as several months. The likelihood of reactivation increases with age and with depressed cellular immune competence. These diseases are monitored by institutions, such as hospitals, where the reporting is as much clinical syndrome as it is by organism. For example, a hospital keeps track of its nosocomial urinary tract infections or ventilator-associated pneumonias. Gonorrhea is the second most commonly reported infectious disease in the United States. Although the disease rate is falling to historic lows, the occurrence of drug resistance is on the rise. Disease Summaries Sexually Transmitted Diseases A Prevalence of common bacterial diseases Approximate incidence (Cases per 100,000 population, United States) Chlamydia 300 200 100 0 Incidence of chlamydial infections is increasing, whereas syphilis and gonorrhea are decreasing Ureaplasma urealyticum Treponema pallidum Neisseria gonorrhoeae Haemophilus ducreyi B Classification of bacterial pathogens Chlamydia trachomatis Gonorrhea Syphilis 96 98 00 Year 02 A B Chlamydia trachomatis major causal agent · C. Transmission is by close personal contact (for example, during birth, or sexual contact). Men develop nongonococcal urethritis and possible other infections (for example, of the prostate or rectum). Women develop infection of the cervix, which may progress to pelvic inflammatory disease. A clinically distinct infection causing adenopathy, with destructive lesions on genitalia and adjacent tissue, is called lymphogranuloma venereum. It uses adhesins to attach to susceptible host cell membrane receptors on mucous membranes. In males, symptoms include Itinfection of the urethra (gonococcal urethritis), purulent discharge, and pain during urination. In females, infection is usually localized to the endocervix, often causing a purulent vaginal discharge. Bacterial proteins (pili to cool temperatures and and outer membrane proteins) enhance the attachment of the bacterium to host epithelial and mucosal cell surfaces, such as those of the urethra, rectum, cervix, pharynx, or conjunctiva, causing colonization and infections. Sexually Transmitted Diseases 369 Sexually Transmitted Diseases G H Treponema pallidum syphilis. Up to ten weeks later, a secondary rash occurs that may be accompanied by systemic involvement, such as syphilitic hepatitis, meningitis, nephritis, or chorioretinitis. In about 40 percent of infected individuals, a tertiary stage occurs after a latent (asymptomatic) period. Tertiary syphilis is characterized by degenerative changes in the nervous system, cardiovascular lesions, and granulomatous lesions (gummas) in the liver, skin, and bones. The has been isolated from endometritis and from vaginal secretions of women who undergo premature labor or deliver low-birth-weight babies. Chancroid is a problem in developing countries, and its incidence is increasing in the United States. Untreated, this progresses to formation of a bubo (a swollen, painful lymph node), which then suppurates.
The rate of diffusion is affected by the size of the particles virus 7th grade science order colcrys 0.5 mg without prescription, temperature infection quotes order generic colcrys on-line, gel viscosity antibiotic vs antiviral order colcrys in united states online, amount of hydration antibiotic examples purchase generic colcrys on line, and interactions between the matrix and reactants. Agarose is often preferred to agar because agar has a strong negative charge, while agarose has almost none, so that interactions between the gel and reactants are minimized. When antibody already present in the gel reacts with the antigen, which diffuses out of the well, a ring of precipitation is formed around the wells. The diameter of the ring is directly proportional to th=e concentration of antigen. The greater the amount of antigen in the well, the farther the ring will be from the well. Key Points Radial immunodiffusion has been used for the quantitative estimation of antibodies and antigens in the serum. It is used to measure: Key Points Immunodiffusion reactions have the following advantages: IgG, IgM, IgA, and complement components in the serum, antibodies to influenza virus in sera, and serum transferrin and -fetoprotein. In this test, the line of precipitation is visible as a band, which can also be stained for preservation. The test can be used to detect identity, cross-reaction, and nonidentity between different antigens in a reacting mixture. Types of immunodiffusion reactions: Immunodiffusion reactions are classified based on the (a) number of reactants diffusing and (b) direction of diffusion, as follows: Single diffusion in one dimension: Single diffusion in one dimension, as the name suggests, is the single diffusion of antigen in agar in one dimension. It is otherwise called Oudin procedure because this technique was pioneered by Oudin who for the first time used gels for precipitation reactions. In this method, antibody is incorporated into agar gel in a test tube and the antigen solution is poured over it. During the course of time, the antigen diffuses downward toward the antibody in agar gel and a line of precipitation is formed. The number of precipitate bands shows the number of different antigens present in the antigen solution. Single diffusion in two dimensions: Single diffusion in two dimensions is also called radial immunodiffusion. In this method, antiserum solution containing antibody is incorporated in agar gel on a slide or Petri dish. The wells are cut on Double diffusion in one dimension: this method is also called OakleyFulthrope procedure. In this method, the antibody is incorporated in agar gel in a test tube, above which a layer of plain agar is placed. During the course of time, the antigen and antibody move toward each other through the intervening layer of plain agar. In this zone of plain agar, both antigen and antibody react with each other to form a band of precipitation at their optimum concentration. Double diffusion in two dimensions: this method is also called the Ouchterlony procedure. In this method, both the antigen and antibody diffuse independently through agar gel in two dimensions, horizontally and vertically. The test is performed by cutting wells in the agar gel poured on a glass slide or in a Petri dish. The antiserum consisting of antibodies is placed in the central well, and different antigens are added to the wells surrounding the center well. After an incubation period of 1248 hours in a moist chamber, the lines of precipitins are formed at the sites of combination of antigens and antibodies (Color Photo 7). Line of precipitation at their junction forming an arc represents serologic identity or the presence of a common epitope in antigens. A pattern of crossed lines demonstrates two separate reactions and indicates that the compared antigens are unrelated and share no common epitopes. In this last case, the two antigens share a common epitope, but some antibody molecules are not captured by the antigen and traverse through the initial precipitin line to combine with additional epitopes found in the more complex antigen.
Purchase colcrys american express. Bonny Silver Socks.
